






It’s a sacred covenant, really, between the doctor and the patient—sick, vulnerable, often needy and at the end of her tether. For her, the idea of the ‘good doctor’ is the only lifeline, and compassion is cure itself. Yet, a mad pursuit of profit now overrides all such ideals, and nowhere is it so blatantly trampled upon as in the business of medical devices, which patients are helpless to resist. It is doctors after all who decide on a procedure. And when that happens, the patient often gets exposed to an unconscionable, well-oiled system of extortion. The margins of profit, for hospitals and doctors—often around 1,000 per cent, or ten times the import price—are truly staggering.
“The Maximum Retail Price of most medical devices is sometimes even 2,000 per cent more than the actual price! An unsuspecting patient has no way out but to pay this highly inflated MRP,” says Dr G.S. Grewal, former president of the Punjab Medical Council and member of the New York Academy of Sciences. “The prices should be fixed only after a full assessment of the manufacturing costs.”
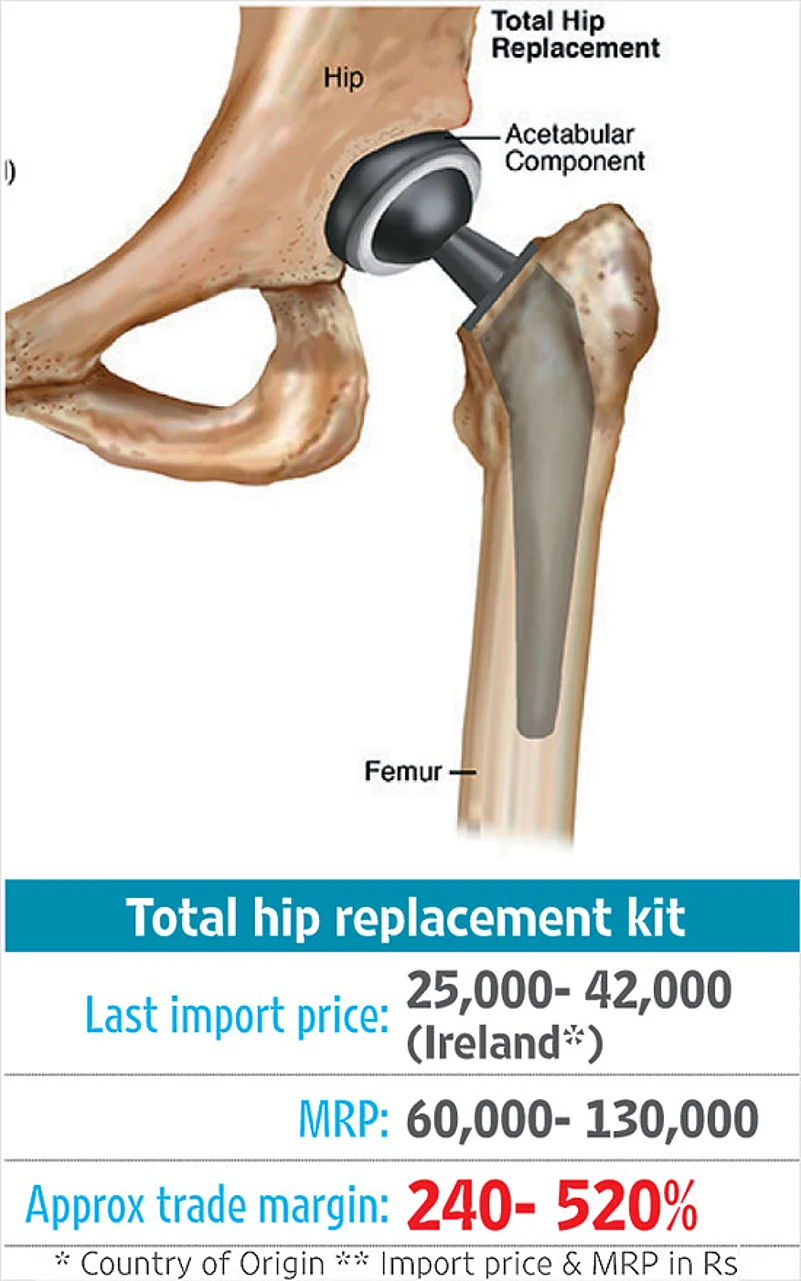
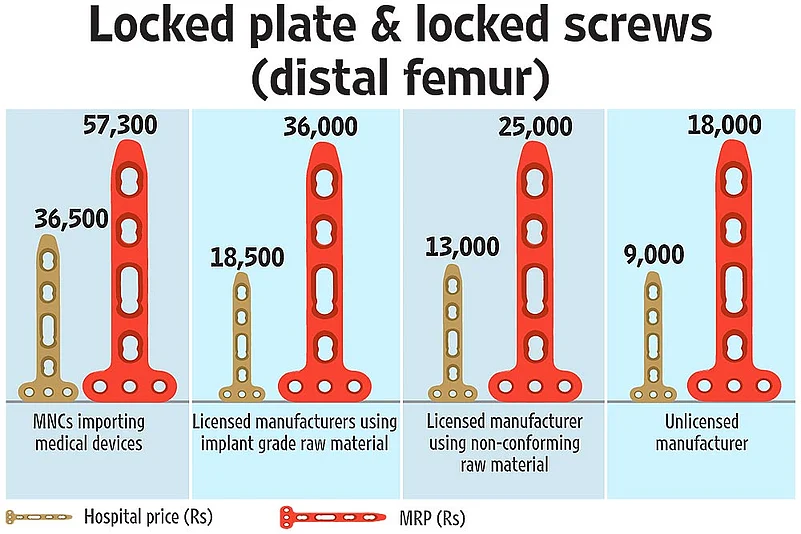
“The cost of a procedure in India is equal to the cost of a car, which is not the case anywhere else in the world,” says Varun Khanna, managing director of the Indian arm of Becton Dickinson, a leading US medical devices company with operations in Haryana. The statement is no exaggeration: patients have to pay exorbitant charges not just for hospital services and facilities, but also medical devices, like hip and knee replacement kits and all implants, most of which are priced 300 per cent to over 1,000 per cent more than the factory gate or import price.




There are no clear guidelines or system of scrutinising surgical procedures and the prescribed line of treatment. Patients are a vulnerable target group for the profiteers. But now, after decades of prices of medical devices being unilaterally decided by manufacturers and medical institutions, some sunlight has begun to fall on this whole infrastructure of greed. The government is beginning to wake up to this phenomenon.
A clear evidence of the wide margins came to the fore in February, when the National Pharmaceutical Pricing Authority (NPPA) gathered information on the prices of cardiac stents, before slashing the MRP by over 75 per cent. The scenario in cardiac care, of course, is only a small screenshot of a much wider reality operating on the same principle. Data compiled by Outlook reveals (see graphics) that in the case of a knee replacement kit (comprising a femoral component, a tibia component and a patella component, besides screws) the MRP fixed by the MNCs is 900 per cent to 1,000 per cent more than the landed cost (the price of an imported product that includes all charges and duties). According to shipment data provided by Bangalore-based Zauba.com (which tracks global trade on basis of bills of shipment), the last landed cost of a knee replacement kit was just Rs 10,159. The MRP was, however, between Rs 95,478 to Rs 1,47, 628, according to suppliers’ bills to hospitals accessed by Outlook. The story is much the same, whether it is hip replacement kit or heart valves, one of the most expensive among imported devices.
Somewhere in the quest for profitability, healthcare industry players are forgetting patients. Take knee replacement surgeries. Last year, an estimated 55,000 such procedures were conducted in India. Depending on the city, the cost varies from Rs 1,10,000 to Rs 2,50,000 at the lowest end and Rs 4,50,000 to Rs 7,00,000 at the higher end in private hospitals.
“In private hospitals there is tremendous pressure to advise tests and surgery. In government hospitals, unless there is deformity or it’s strictly required, we do not advise knee replacement,” states a senior orthopaedic surgeon, who feels at least 20 per cent of such surgeries are unnecessary.
The surgeon points out that in leading government hospitals like AIIMS or Safdarjung in the capital, the cost of a knee replacement is around Rs 75,000, though they use the best imported implants, just like in private hospitals. The fact that government hospitals get the kits at competitive prices, far below massively inflated MRPs, through a bidding process carried out every two years to allow for model changes, helps patients. In most private hospitals, the patients are forced to buy from the hospital, which keeps at least a 20-30 per cent margin.
“We opted for Safdarjung Hospital when my wife needed knee replacement after she damaged the cartilage in a fall nine years back and was unable to walk. We did not have insurance and had to arrange money for the costly operation. We also chose Safdarjung as they have very experienced surgeons,” says Pinaki Dasgupta, a Delhi-based designer. Expressing satisfaction with the results, Dasgupta says if needed, he’d choose Safdarjung Hospital again, “given the quality of service and expertise of doctors there”, not to speak of the inflated bills in private hospitals. He should know, for he has had to pay a six-digit fee for his wife’s recent hospitalisation, which was not fully covered by insurance.

Probir Das, a board member of Medical Technology Association of India (MTai, which represents major global firms), justifies the margins, especially at the hospital end. “If hospitals don’t have a positive outlook of viability, how can we have one? I am not speaking in favour of hospitals but that of patients. If hospitals don’t add more beds, how will patients get better care?” MTai has urged the government to adopt a more “nuanced approach in its policy-making mechanisms”, considering the capital-intensive nature of the medical devices sector. What Das suggests through business-speak is that hospitals should make huge profits for them to offer more beds to patients.
What is the remedy, then, for a public groaning under high medical costs? Can, at some point, these prices be regulated and capped? So far, only four medical devices have been brought under a price ceiling as per the Drug Price Control Order (DPCO), by virtue of being placed among the national list of essential medicines. They are among 23 medical devices the government has either notified as ‘drugs’ or is regulating as per the Drugs and Cosmetics Act (D&C Act), says Bhupendra Singh, NPPA chairman. It’s under the same law that the NPPA is monitoring the remaining 19 medical devices that contain pharmacologically active substances. Unless classified as drugs, the medical devices don’t come under NPPA’s purview. Officials say there is a need to expand the list of medicated devices that must be treated as drugs.

After month-long consultations with MNCs and Indian manufacturers, the NPPA last month formalised the framework under which data—on the margins given to distributors, hospitals and the final selling price—is being collected.
Yet, significantly, even a national regulatory agency has to make glaring compromises when it comes up against a strong business group. Just days ahead of the rollout, the companies got the NPPA to drop the requirement for furnishing information on the factory gate and landed cost of imported devices—two vital bits of information that would help track the wide trade margins subsumed in the MRP. Initially, the firms had agreed, but later they had many reservations, official sources stated. The firms have, in the interim, been directed to state the MRP on all products and not to raise the end-user price by more than 10 per cent annually.
“We are still in the process of collecting information from companies about prices and as of now there is no plan to fix ceiling prices of any other medical devices,” Singh says. “Price fixing is an intrinsic process and each medical device market has a different business model and manufacturing portfolio.”
Over 14,000 different product types, like adhesive bandages, drug delivery devices, diagnostics, implants, stair-walking wheelchairs, robotic surgical systems and magnetic resonance imaging devices, all come under medical devices, according to Global Medical Device Nomenclature (GMDN).
Unlike generic drugs, India has a meagre 1.3 per cent share in the $342.39 billion global medical devices market. Despite allowing 100 per cent FDI to promote domestic manufacturing, India’s import dependency is as high as 70-90 per cent across various categories of medical devices and even components for domestically produced products. For example, devices such as heart valves and knee caps are completely controlled by MNCs in India, while over 70 per cent of intraocular lenses are indigenously produced and are priced more competitively.
Pritam Datta, research associate, Public Health Foundation of India (PHFI), feels the need for a thoroughgoing approach. “How far the NPPA initiative is sufficient is a questionable issue,” he says. Based on his research, Datta says most of these scheduled or notified devices are, in a sense, ‘consumed’ by patients—as in, implanted. Some 46 per cent of imports are of diagnostic equipments or unscheduled medical electronics—ultrasound scanner, UV/IR apparatus, X-ray tube, MRI et al. “Most of these are overpriced in the Indian market. India needs a comprehensive price regulation for all medical devices and equipment used here,” he stresses.
Add to this the lack of, and resistance to, any means to ‘audit’ the line of treatment adopted by doctors, and the rise in surgical interventions or procedures—all of which leaves patients totally at the mercy of a profit-driven system.
Health activist Ashok Kumar Bhargava puts it in perspective. “The turnover of surgical devices companies is today three times that of pharmaceutical companies,” says Bhargava, who has been striving for over 20 years to persuade the government to promote use of generic medicines and ensure checks and balances to make healthcare more affordable. Before prices were capped recently, it was estimated that high-priced cardiac stents yielded Rs 3,500 crore a year to MNCs—more than enough to be able to bribe and coerce doctors into making certain choices. With no scrutiny or system in place to monitor the need for a procedure, the number of stents implanted has spiralled in recent years—industry estimates put it at 4.75 lakh every year.
The desirability of stents needs to be judged against other options in unbiased medical terms. But prices are obviously a factor that dictates doctors’ choices. “There is a minimum of 30 per cent commission fixed or the hospitals and stores will not stock or display your company products. In the case of hospital supply, the choice is swung by the largest commission,” says Bhargava, explaining how Indian makers of medical devices, or dealers of imported devices, are hand-in-glove with hospitals. He wonders why the government has so far failed to bring commonly used medical devices under the Essential Commodities Act and price control, and scrutinise all lines of treatment and procedures.

Many activists, including “ethical” medical practitioners, have been waging an arduous battle on these fronts for decades. Despite India emerging as a major medical tourism hub, healthcare within the country presents a picture of manufactured scarcity. The healthcare cost is such that one major illness or accident in the family is often enough to spell financial ruin, particularly if one has to seek private medical care.
Pricing practices in India are not very different from that of other countries—in the UK, manufacturers are free to set prices, except for products classified as pharmaceuticals (or drugs) that are subject to supply-side control by the Department of Health’s Pharmaceutical Price Regulatory Scheme (PPRS). But there’s a big difference. The Primary Care Trusts (PCTs), responsible for providing optimal care across primary, secondary and community healthcare services within the prescribed budget, has to keep a tight rein on things. So the PCTs negotiate and set prices with device manufacturers. Similarly, the UK’s iconic National Health Service (NHS) has checks and balances in place to evaluate and assess the costs and effectiveness of medical technologies used in the care of patients. In India, however, with the public health system unable to cope with the growing demand, there’s ample room for manufacturers, distributors and hospitals to prosper.
Some changes are hopefully in the offing. For one, there are expectations that ultimately all medical devices may come under price control, a move feared by MNCs. Alarmed MTai members, true to form, paint a dire picture, warning that it would have an adverse impact on healthcare in India as manufacturers would be forced to withdraw or withhold many latest products from the market.
Health officials, however, clarify that any such attempt would be to check “only profit in trade margin”. “We don’t touch the margins of the companies. The high trade margins don’t go for R&D but in promoting and marketing a product,” says an official.
For better monitoring of medical devices, the software of the Integrated Pharmaceutical Database Management System (IPDMS), earlier known as pharma databank, is in the process of being modified and tailored to collect information. It has already been updated to collect information on stents.
In January, the Union health ministry notified the medical devices rules, which will come into effect from January 2018, under which Indian manufacturers, but not foreign ones, are to undergo audit by notified bodies. Official sources admit it’s doubtful if they have full data of medical devices licensed in the country; some devices don’t even need a DPCO license.
“We are not fixing prices. We can only monitor,” says a senior health ministry official, adding that no study has so far been commissioned to find out the manufacturing cost of various products in the country or in overseas markets. Besides the firewall of “confidential data”, officials say MNCs can easily manipulate data through their Indian subsidiaries. “Even if we get the data, it would be hard to authenticate it, as they could manipulate the price at which they supply to hospitals or healthcare providers overseas.”

Must devices be defined as ‘drugs’ to rationalise their pricing? No, a task force set up by the Department of Pharmaceuticals had recommended the opposite in a report submitted in 2015. The report, still awaiting implementation, states: “Once the proposed exclusion of medical devices from the definition of drugs…is implemented, the medical device may be included separate from drugs in the Essential Commodities Act and regulated under a separate medical devices (price control) order”. The task force had recommended that the NPPA be empowered to monitor prices of medical devices under a separate vehicle.
Among its other suggestions was to “create enough opportunity to provide appropriate returns on investment for all stakeholders” and to “liaise with IRDA and the health insurance industry to cover new technology on risk-based pricing models”. The most forward-thinking of its suggestions was that “taxes should be levied with reference to the MRP as a disincentive to peg MRP at a very high level”. Currently, taxes are levied at the factory gate price or landed import price, which leaves ample room for companies to fix MRP at sky-high levels. And given the power of MNCs to bribe doctors and sway their choices, the decision between an Indian implant and an imported product is hardly ever made on the basis of what’s best for the patient.
At a time when hospitals can, theoretically, find a way around price controls over devices, what does one do? “The NPPA has no control on procedure costs,” says Malini Aisola, a health activist with the All India Drug Action Network. “The health ministry has to do something about regulating procedure costs in hospitals because they have a free hand to charge anything they want. Right from consulting fee or procedure cost or the package cost, hospitals charge at will. Whether it’s a caesarean, an appendectomy or angioplasty, the costs vary across hospitals. In the case of stents, they have repackaged the costs and there is no transparency.”
Khanna of Becton Dickinson says “capacity creation” through government procurement could bring down prices. Some states have adopted this mode with improved outcomes. But beyond procurement of medical devices through a government system, there is need to fix the price of the various procedures that require these devices, bring all medical decisions and records under scrutiny, as in the US, and levy taxes on the MRP to disincentivise high prices and make healthcare more affordable. In the absence of the long promised universal healthcare system, that is the least the government can do.
A widely-accepted, modern version of the Hippocratic Oath urges doctors to remember that they treat not “a fever chart or a cancerous growth, but a...human being, whose illness may affect the person’s…economic stability”. We hope they pass on this piece of wisdom to hospital managements, if not to their cohorts among dealers and importers.















